We talk about autoimmune disease as a problem of biology — and it is. The immune system, which exists to tell self from non-self, stops being able to. But before it becomes a problem of biology, it is a problem of information. The disease leaves a long, detailed trail. The system records almost none of it.
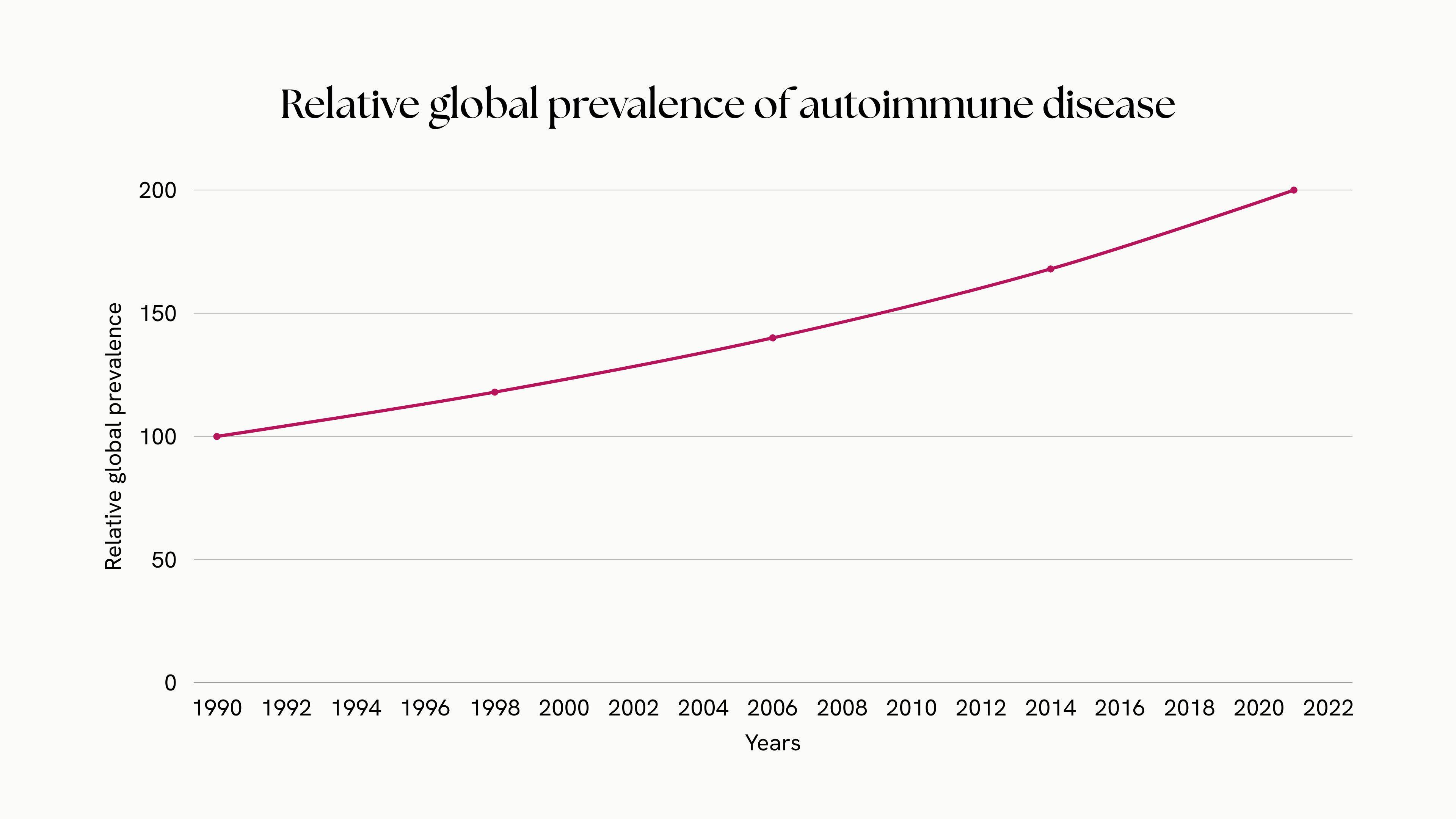
This matters more than it sounds, because it changes where the most useful work is. Autoimmune conditions affect an estimated 5–10% of the population in developed countries — in the largest study to date, a UK cohort of 22 million people, around one in ten.1 And the trend is not flat. Global prevalence has roughly doubled over three decades, and the curve is still pointing up.2
Much of the effort to help these patients is waiting on better science. Some of it isn’t. Some of it is waiting on something more ordinary: writing the right things down.
01 The years before a name
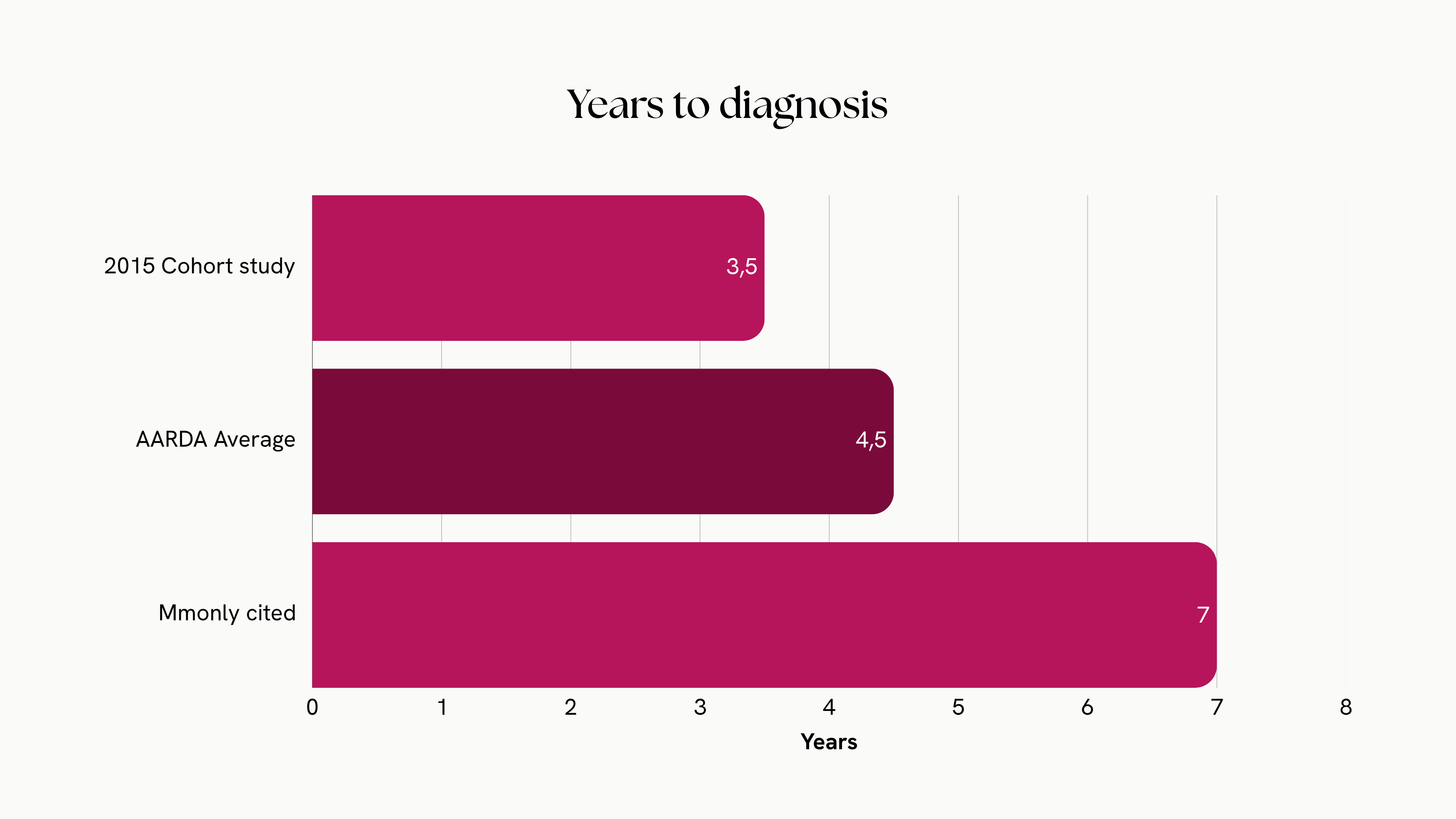
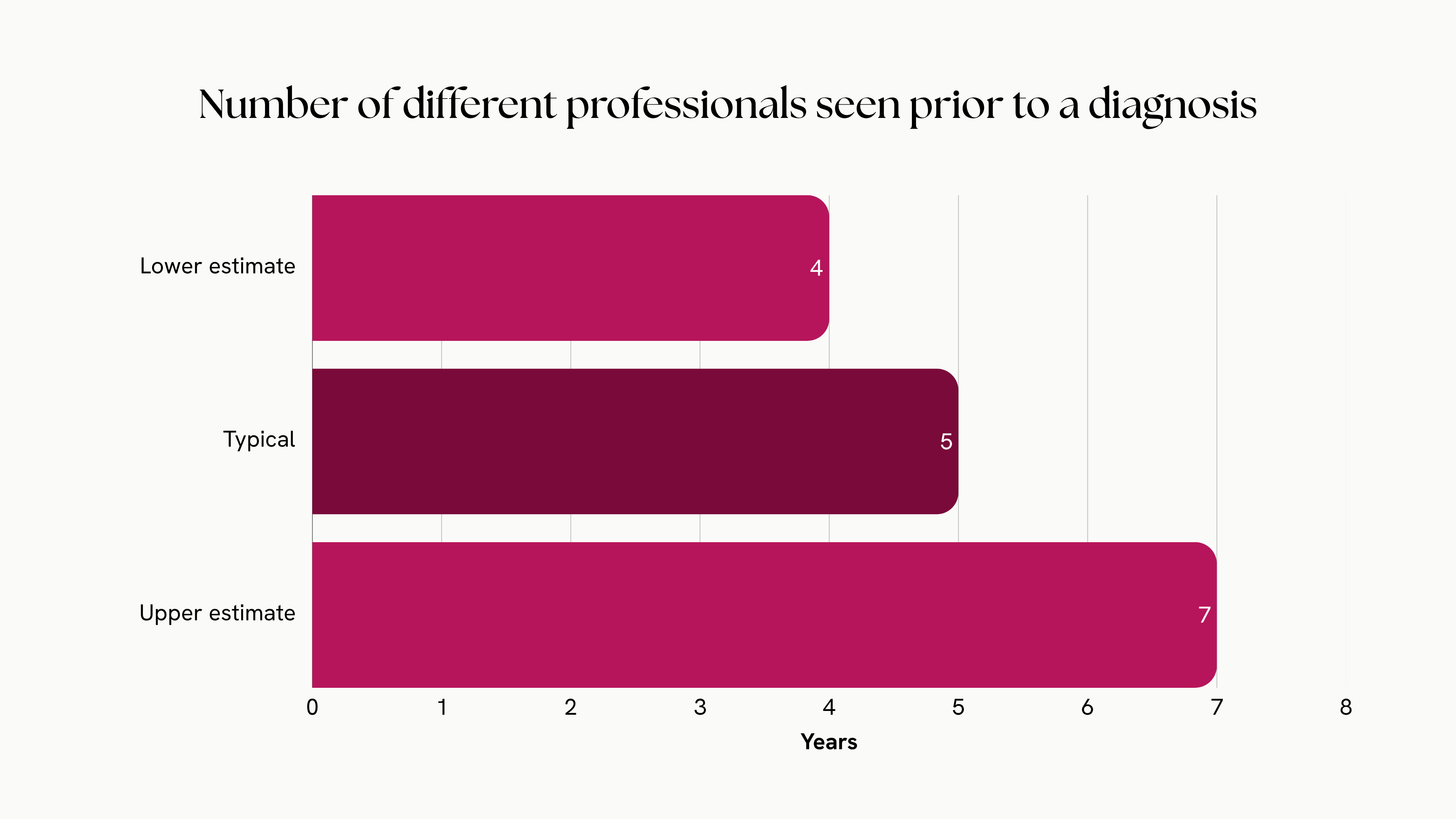
A person in the early stages of an autoimmune disease does not arrive with a clear question. They arrive with fatigue, with joint pain, with a rash that comes and goes, with numbers that look normal in isolation. Getting from that first appointment to a diagnosis takes years, and several doctors along the way.
That delay is usually framed as a purely clinical problem: the symptoms are vague, they overlap with everything, autoimmune disease is genuinely hard to recognise early. All true. But there is a second cause underneath it that gets far less attention. The information needed to shorten that path mostly does not exist in a usable form — not because no one lived it, but because no one captured it.
02 A disease that happens between appointments
Autoimmune conditions fluctuate. They flare and remit, sometimes over weeks, sometimes within a single day. The clinically meaningful events — when symptoms first appeared, what seemed to set them off, how long a flare lasted, what the body looked like in the quiet stretches in between — happen at home, not in the consulting room.
What the system records is the opposite of continuous: a snapshot, taken on the day of the appointment, of how the patient happens to feel in that moment and what they can remember. And recall is unreliable in a specific, well-documented direction. A patient who feels well on the day of a visit tends to remember the preceding weeks as milder than they actually were.5 So the most informative part of the disease — its movement over time — is also the part least likely to survive into the record.
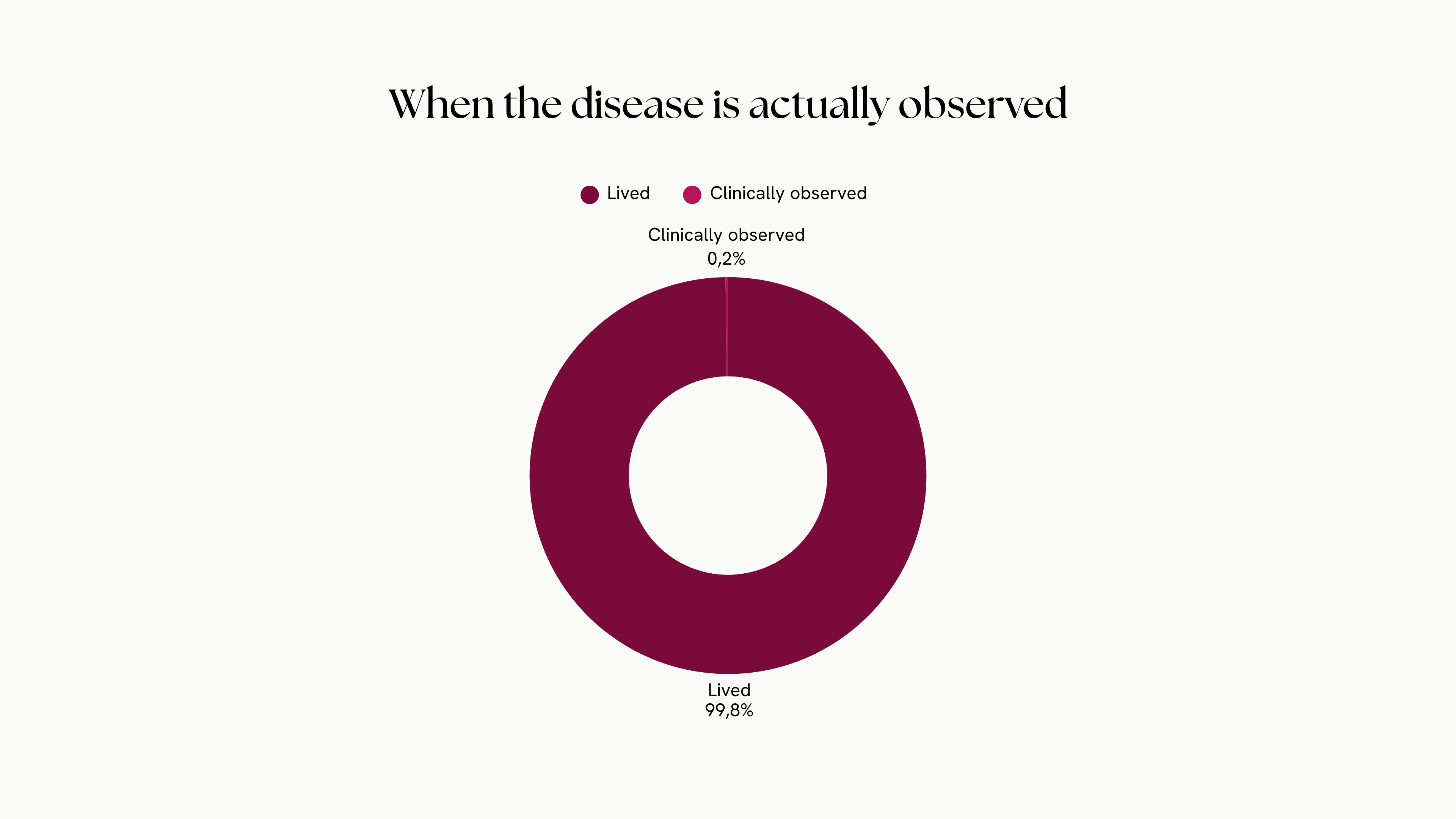
The most informative part of the disease is its movement over time. It is also the part least likely to be written down.
03 Fragmentation
Even the information that does get captured rarely sits in one place. Autoimmune disease is multi-systemic by nature, so a single patient may move between a rheumatologist, a dermatologist, a gastroenterologist and a GP — each holding a fragment, each in a different system, in a different format, none designed to talk to the others.6 The result is not one continuous record of a life with the disease. It is a scattered set of episodes, held by custodians with no efficient way to cooperate.
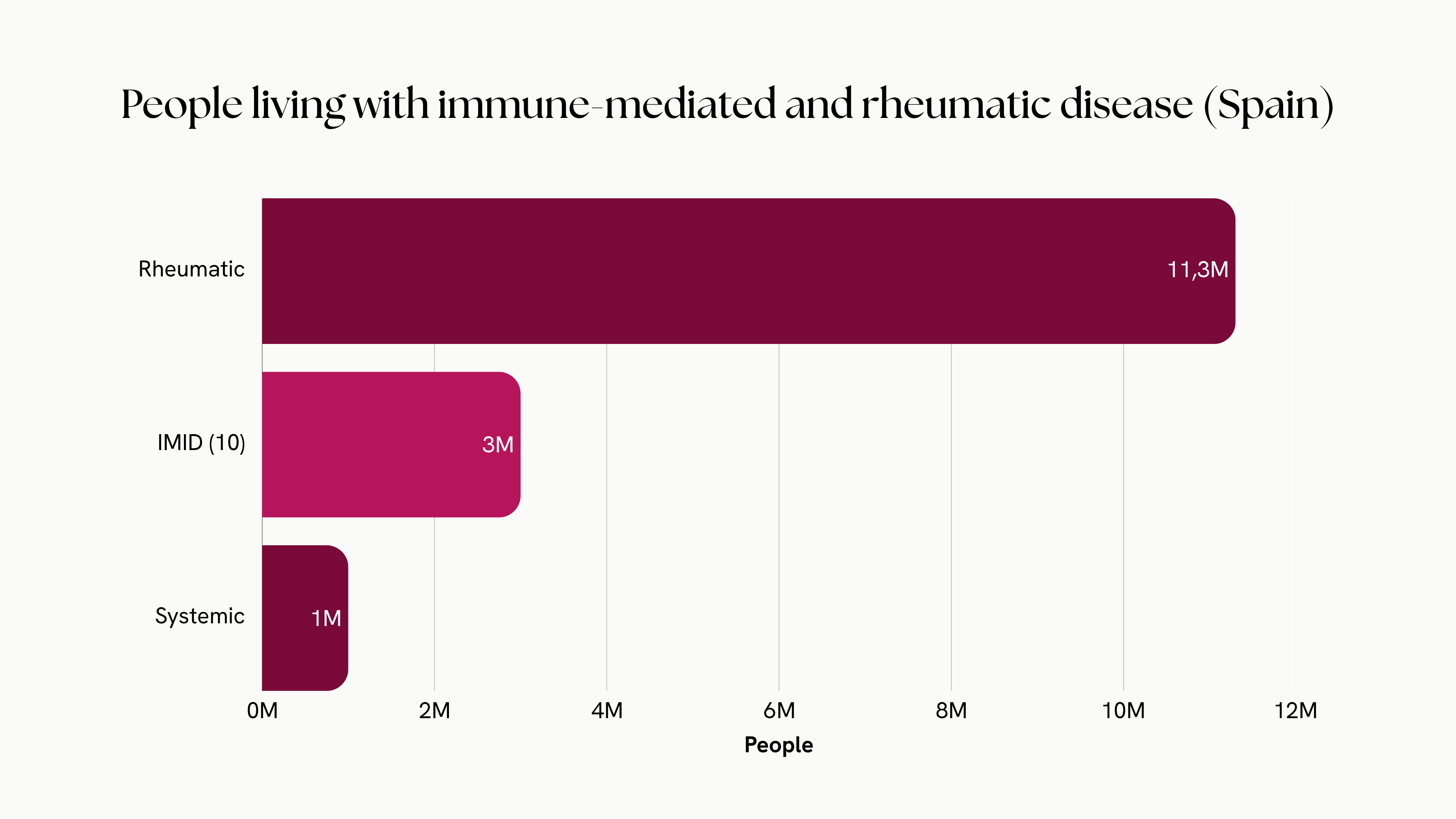
The scale of that scattering is easy to underestimate. In Spain alone, rheumatic disease touches more than one in four adults; systemic autoimmune disease, around a million people. The capacity meant to hold all of that context is a different order of magnitude entirely.
One specialist per ~49,800 inhabitants — below the recommended minimum, with three of four services struggling to fill vacancies and 16% of the workforce retiring this decade. The context a patient generates over years has almost nowhere structured to land.7
And the fragments are not independent. In the UK cohort, autoimmune conditions co-occurred far more often than chance would predict — having one raises the odds of developing another.1 That is the strongest argument there is for treating autoimmune disease as a single connected category rather than a set of unrelated silos. You cannot see the pattern if every fragment lives in a different file.
04 Why this is also a research problem
This is not only a problem for the person waiting for a diagnosis. It is the same problem, one level up, for everyone trying to study these diseases.
Real-world evidence depends on structured data about what actually happened to patients: symptom severity, functional status, relapse rates, changes in biomarkers over time. For autoimmune disease, that is often precisely what is missing — not because patients didn’t experience it, but because it was never recorded in a structured, comparable way.8 You cannot study, at scale, what was never written down. The information problem at the bedside becomes the information problem in the cohort.
It is also where the market is moving. Clinical decision support is the fastest-growing segment of European digital health, and the capital that remains after the sector’s correction is flowing toward structured data and decision tools rather than apps.9 The companies that arrive with rigorous, structured, regulation-ready data will hold positions that are hard to displace. The constraint, again, is not storage. It is structure.
05 What “solving it” actually means
It is tempting to describe all this as a gap that the right app closes. It isn’t — or not only. The hard part is not building somewhere to put the data. It is capturing the right data, from the right source, in a structure that still holds up when you later try to study it. That means three things at once.
Get those three right and the same information serves the patient in the consulting room and the researcher in the cohort: one record, read at two scales.
06 Where we stand
None of this is solved by stating it clearly. It is infrastructure, and infrastructure is slow: it has to earn trust from patients, fit how clinicians already work, and meet a standard of rigour that research can rely on. We are building toward it deliberately rather than quickly, and we would rather be honest about the distance than oversell the arrival.
But the framing matters, because it decides what you build. If autoimmune disease is only a biological problem, you wait for better science. If it is also an information problem — and it is — then some of the most useful work available right now is more ordinary, and more within reach, than it first appears: recording the right things, in the right structure, before the science that will need them arrives.
Neural Omega is building infrastructure for autoimmune disease — from patient-facing tracking to research-grade study design. The Observatory is where we think out loud about the problem.